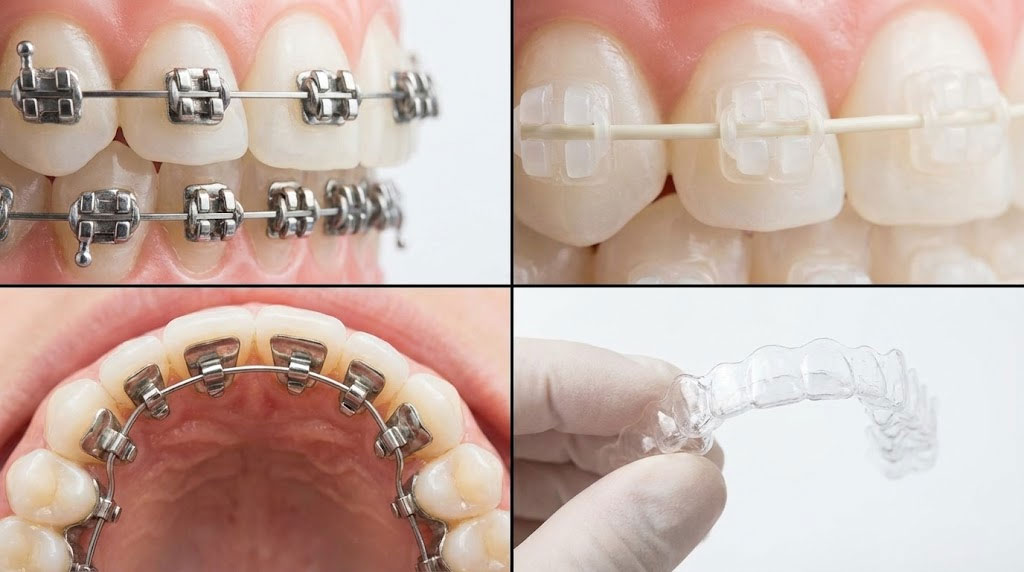

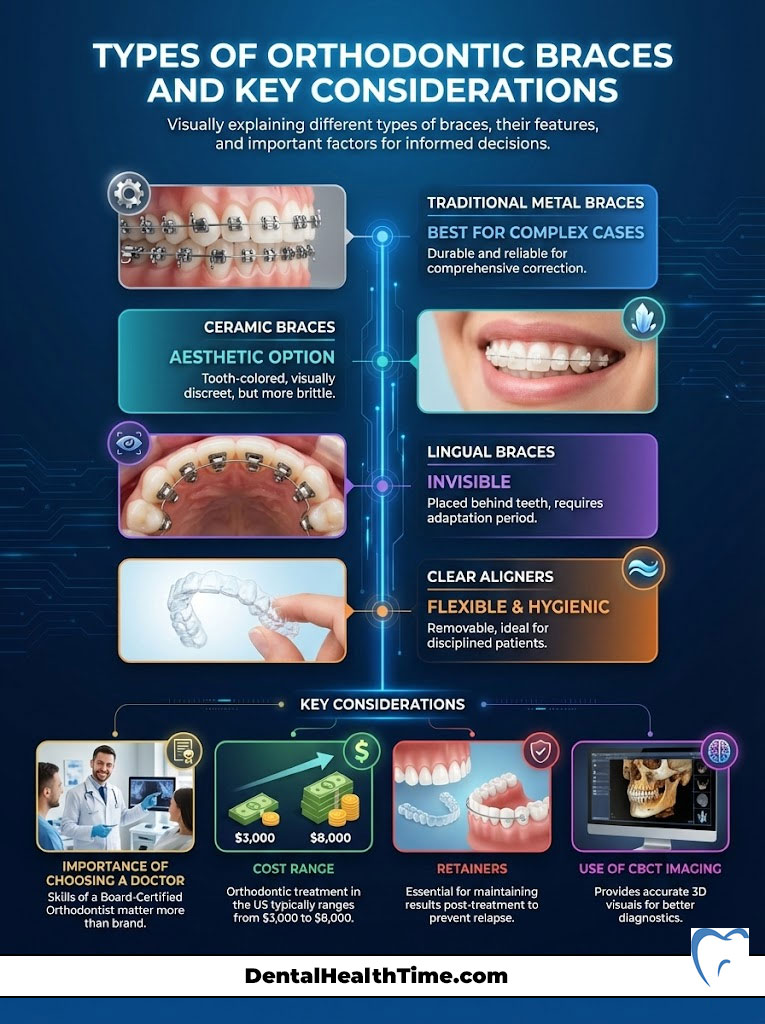
When patients ask, “What are the different types of braces?” the answer falls into four primary clinical categories. Traditional metal braces are the standard for complex bites and offer the highest durability. Ceramic braces provide a translucent aesthetic by using tooth-colored polycrystalline alumina. Lingual braces are truly invisible because they are bonded behind the teeth on the tongue side. Finally, clear aligners (such as Invisalign) use removable plastic trays for a wire-free approach. Your specific biological diagnosis and lifestyle needs dictate the best choice.
The Evolution of Modern Smile Design
Orthodontics has shifted dramatically in the last two decades. We used to focus strictly on “correcting” crooked teeth. Today, we practice dentofacial orthopedics. This means we are not just lining up enamel.
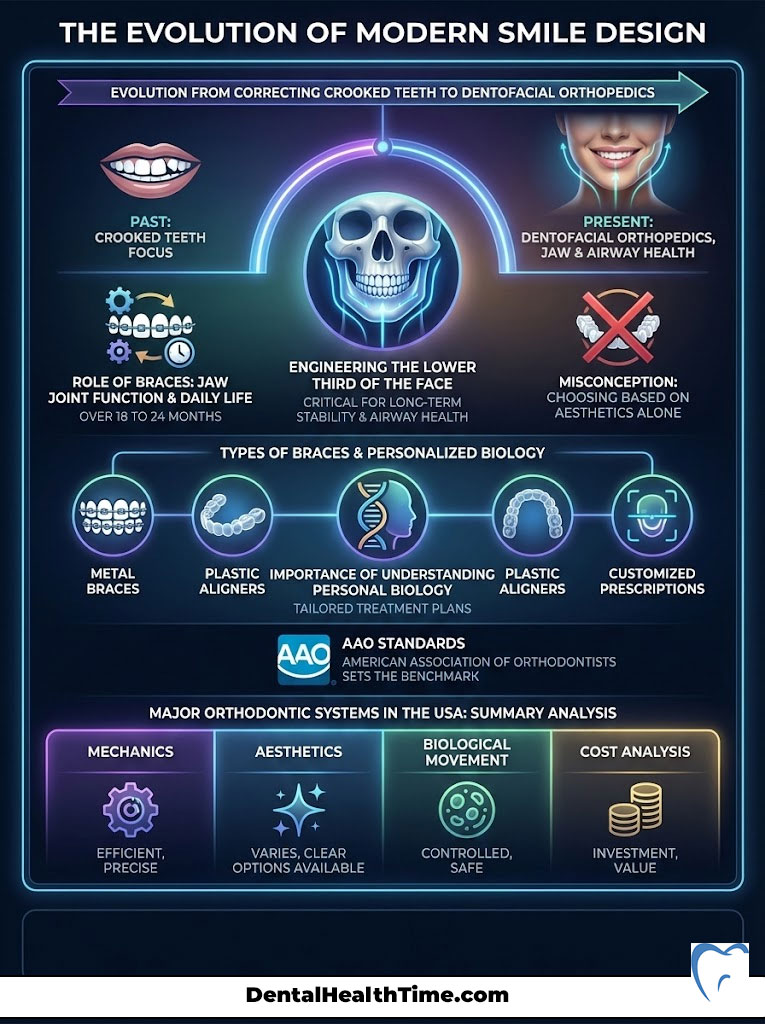
We are engineering the lower third of the face. Our goal is to ensure long-term stability, airway health, and facial balance. Choosing an appliance is a significant medical decision. It impacts your daily life for 18 to 24 months.
It also dictates how your jaw joints function for the rest of your life. Many patients walk into my clinic assuming they just need to pick a color. But the reality is more complex. When patients ask, “What are the different types of braces?” they are often surprised.
The answer involves more than just metal or plastic. It involves a customized prescription for your unique biology. A plastic tray pushes teeth differently than a steel wire pulls them. Therefore, the “best” type is not always the one that looks the best.
It is the one that can physically achieve the movements your bone structure requires. As a Board-Certified Orthodontist, my goal is to guide you past the marketing hype. We need to look at the physics. We need to look at the biology.
This guide adheres to standards set by the American Association of Orthodontists (AAO). We will cover the mechanics and the aesthetics. We will also cover the biological movement and the cost analysis of every major system available in the USA today.
Key Statistics in Orthodontics
- 4 Million: The approximate number of Americans wearing braces at any given time.
- 25%: The percentage of orthodontic patients who are adults (over age 18).
- 18-24 Months: The average treatment duration for comprehensive cases.
- $3,000 – $8,000: The typical cost range for orthodontic treatment in the US without insurance.
- 7 Years Old: The recommended age for a child’s first orthodontic screening.
- 95%: Success rate of cases when patient compliance is high.
The Diagnostic Foundation: How We Choose Your Appliance
Before we discuss hardware, we must discuss diagnosis. In my practice, the specific type of brace is secondary to the treatment plan. You can buy the most expensive Ferrari engine.
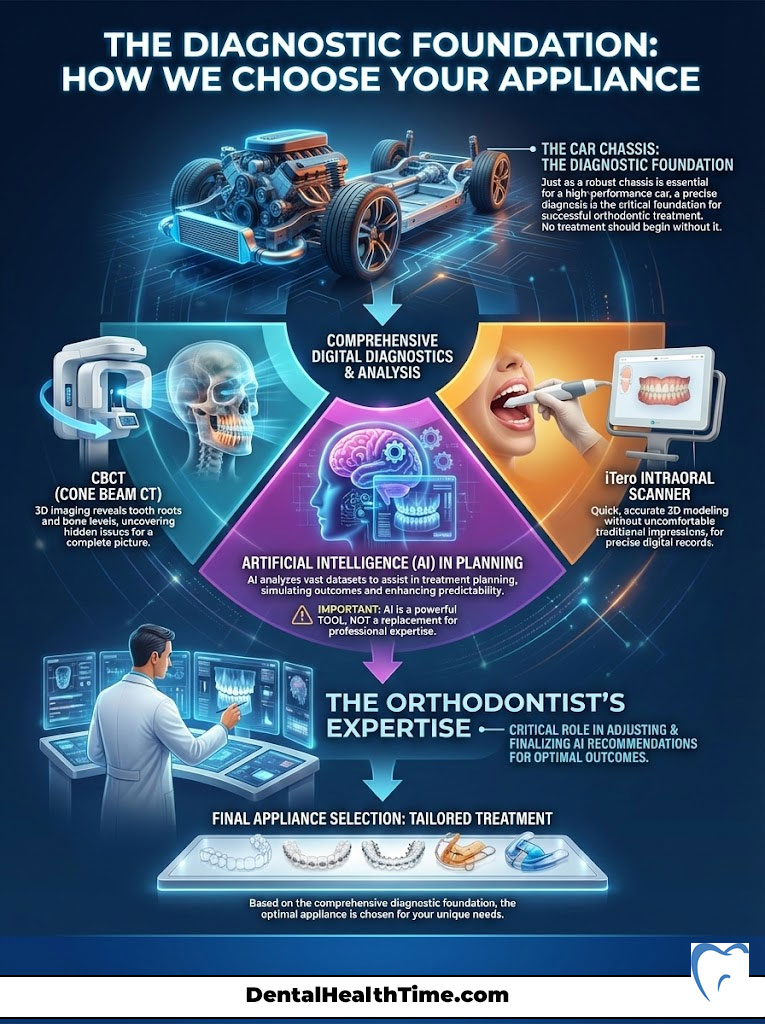
But if the chassis is bent, the car won’t drive straight. The same logic applies to your mouth. We cannot plan your treatment just by looking at your smile. We need to see what is happening under the gums.
This is why comprehensive records are non-negotiable. According to the American Board of Orthodontics (ABO), a proper diagnosis requires evaluating the roots. We must also check bone levels and the jaw joints (TMJ).
Digital Diagnostics: CBCT and iTero
Modern orthodontics relies heavily on Cone Beam Computed Tomography (CBCT). This is a specialized 3D X-ray. It allows us to see the exact position of tooth roots relative to the sinus floor.
We can also see proximity to nerve canals. We also use iTero digital scanners. These wands capture thousands of images per second. They create a 3D model of your teeth instantly. We no longer use that gooey impression material that makes everyone gag.
The Role of Artificial Intelligence
AI has entered the chat. We use software to simulate tooth movement before we bond a single bracket. For example, when planning clear aligners, the software helps us predict collisions.
However, AI is a tool. It is not the doctor. It often underestimates the force needed to rotate a canine tooth. That is where the orthodontist’s expertise comes in. We must override the computer’s suggestion to ensure clinical success.
The Biological Reality: How Teeth Actually Move
Regardless of “What are the different types of braces?” you choose, the biology is the same. We are stimulating an inflammatory response. This is a physiological process.
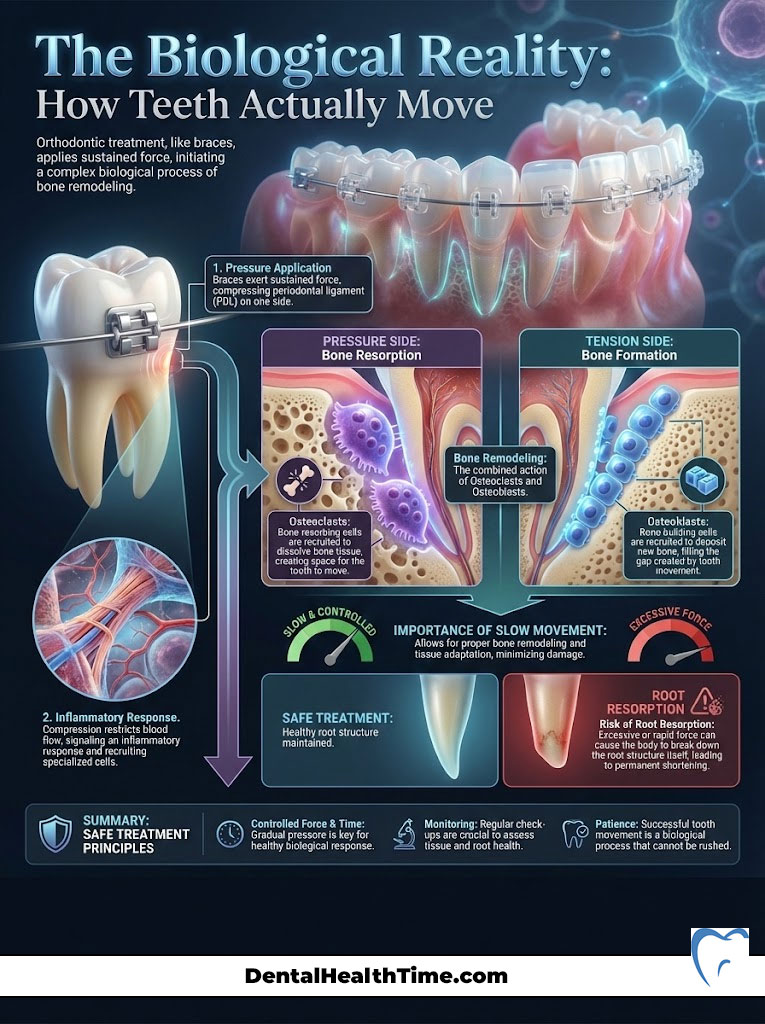
Bone Remodeling
When a brace puts pressure on a tooth, it constricts blood flow on one side. This signals the body to send cells called osteoclasts. These cells eat away the bone in the path of movement.
On the other side, tension is created. Cells called osteoblasts rush in to build new bone here. This process is called bone remodeling. It takes time. It cannot be rushed.
The Rate of Movement and Root Resorption
Patients always want faster treatment. But faster isn’t better. Faster can be dangerous. If we apply too much force, the body might attack the tooth root.
This is called root resorption. It means the roots get shorter. Once a root is shortened, it never grows back. This is why slow and controlled movement is the hallmark of a safe treatment plan.
Traditional Metal Braces: The Clinical Gold Standard
Despite the influx of new technology, traditional metal braces remain the workhorse of our industry. When a case is complex or surgical, metal is king. It is often the only tool precise enough to get the job done right.
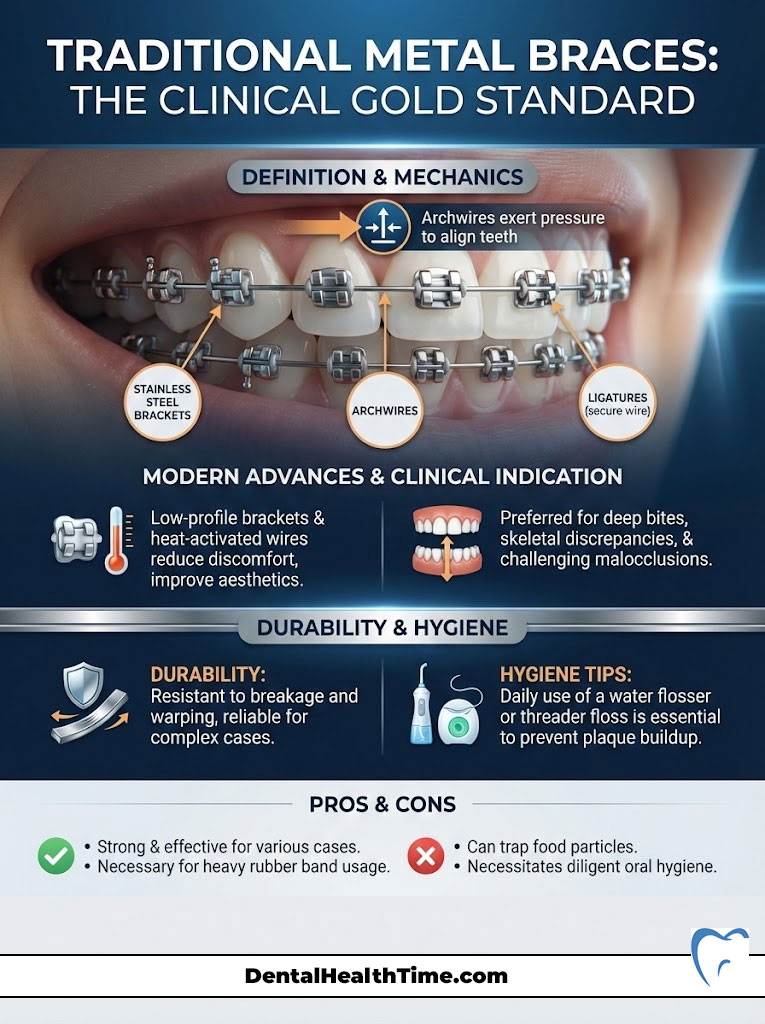
Definition & Mechanics
This system relies on three components. First, high-grade stainless steel brackets are bonded to the center of each tooth. Second, the orthodontic archwire acts as the engine.
The wire wants to return to its original U-shape. As it does, it drags the teeth along with it. Third, ligatures hold the wire into the bracket slot. These are the small rubber bands that kids love to color-coordinate.
Modern Advancements
Forget the “metal mouth” insults from 1990s sitcoms. Modern brackets are “low-profile.” This means they are physically smaller. They sit flatter against the tooth.
This reduces lip irritation significantly. The metallurgy has also improved. We use heat-activated nickel-titanium wires. These apply gentle and constant pressure over weeks. This avoids the heavy and painful forces of the past.
Clinical Indication: Why Doctors Love Them
We prefer metal for malocclusion correction involving deep bites. They are also superior for skeletal discrepancies. Metal does not break. It does not warp.
If we need to pull a customized canine tooth down from the palate, metal provides the strength. They are essential for correcting Class II (overbite) cases. They handle the heavy rubber bands required for these movements.
Pro Tip: The Hygiene Factor
Metal braces are durable, but they trap food. You must use a water flosser or threader floss daily. Plaque accumulation around the bracket can lead to “white spot lesions.” These are permanent scars on the enamel that remain after the braces come off.
Pros & Cons
- Pros: Most cost-effective option. Extremely durable materials. Zero compliance required. Precise control over roots.
- Cons: Highly visible aesthetics. Difficult to floss between wires. Can irritate inner cheeks initially.
Ceramic Braces: Aesthetic Orthodontics for Adults
For patients who need the control of fixed appliances but refuse the “train track” look, ceramic braces are the answer. They function almost exactly like metal braces. But they trade stainless steel for a glass-like material.

Material Science: Polycrystalline Alumina
These brackets are made from Polycrystalline Alumina. This material is either translucent or clear. It blends with the natural tooth shade. Brands like Clarity Advanced are designed to be matte.
They do not reflect light like metal does. When paired with a coated “white” wire, the system becomes very discreet. It is hard to see from a normal conversation distance.
Durability vs. Aesthetics
There is a trade-off. Ceramic is harder than enamel. But it is more brittle than steel. Steel bends under pressure.
Ceramic can fracture or shatter. This makes them slightly more fragile. If you play contact sports like wrestling, we usually recommend a mouthguard. We might also suggest metal brackets to prevent breakage.
Staining Myths vs. Reality
A common question regarding “What are the different types of braces?” concerns stains. High-quality ceramic brackets do not stain. They are impervious to tomato sauce or coffee.
However, the clear elastic band that holds the wire does stain. If you eat curry on Tuesday, those bands will turn neon yellow. The good news is that we change those bands at every appointment.
Clinical Note: The Deep Bite Risk
Because ceramic is harder than tooth enamel, we have to be careful with “deep bites.” This is where top teeth cover bottom teeth excessively. If your top teeth bite down onto the bottom ceramic brackets, damage occurs.
The brackets will act like sandpaper. They will wear down your natural tooth structure. In these cases, we might place metal on the bottom teeth. We then place ceramic on the top for aesthetics.
Self-Ligating Braces: The Damon System and Speed
Self-ligating braces look similar to traditional metal or ceramic braces. But the engineering under the hood is totally different. They do not use elastic rubber bands to hold the wire.
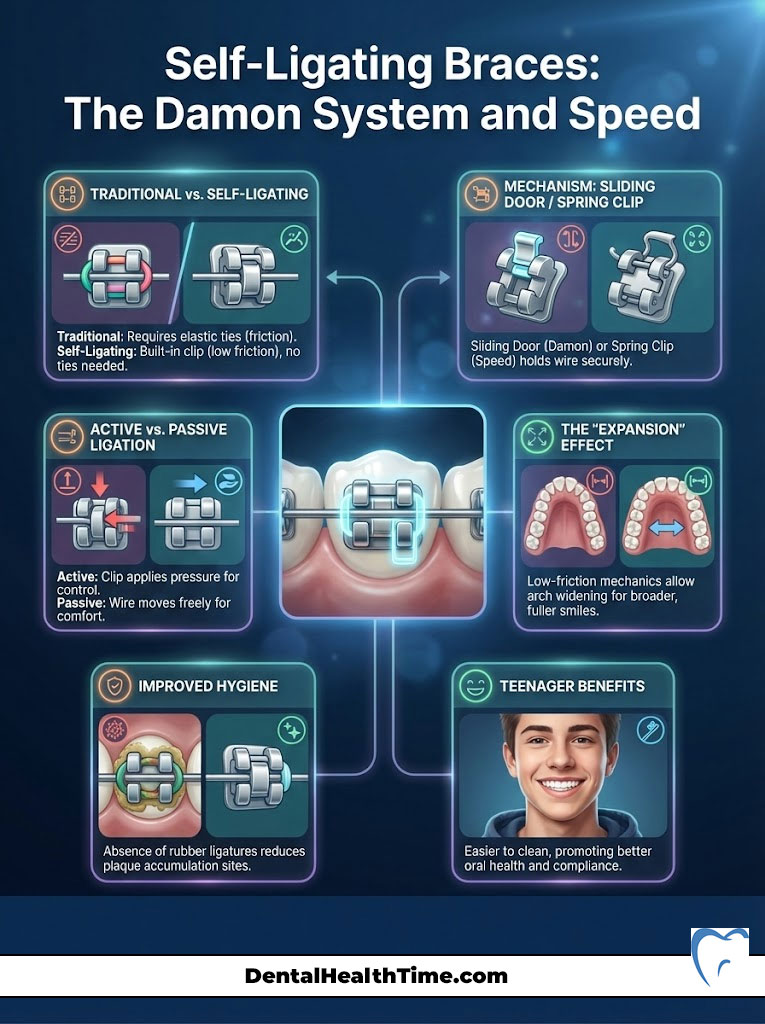
The Mechanism
Instead of a rubber band, these brackets have a built-in “sliding door.” Some use a spring clip. The orthodontist presses on the wire.
The door snaps shut to secure it. This creates a tube for the wire to pass through. It changes the physics of tooth movement.
Active vs. Passive Ligation
This is where physics gets interesting.
- Passive Ligation: The wire floats freely inside the bracket slot. This dramatically reduces friction. Lower friction means we can use lighter forces. This is biologically healthier for the roots.
- Active Ligation: The clip presses against the wire. This provides more control. It is usually used in the finishing stages of treatment.
The “Expansion” Effect
We often use self-ligating systems for patients with narrow smiles. The low-friction mechanics allow the archwires to broaden the dental arch. This happens naturally.
This can give a wider and fuller smile. It reduces dark corridors at the corners of the mouth. It often avoids the need for a rapid palatal expander in borderline cases.
Hygiene Benefits
Since there are no rubber ligatures, plaque has nowhere to hide. Self-ligating braces are generally easier to keep clean. This is a massive benefit for teenagers who struggle with brushing.
Lingual Braces: The Only True “Invisible” Option
If visibility is your absolute deal-breaker, lingual braces are the superior choice. Unlike aligners, which still have a sheen, lingual braces are hidden. They are bonded to the back of your teeth.
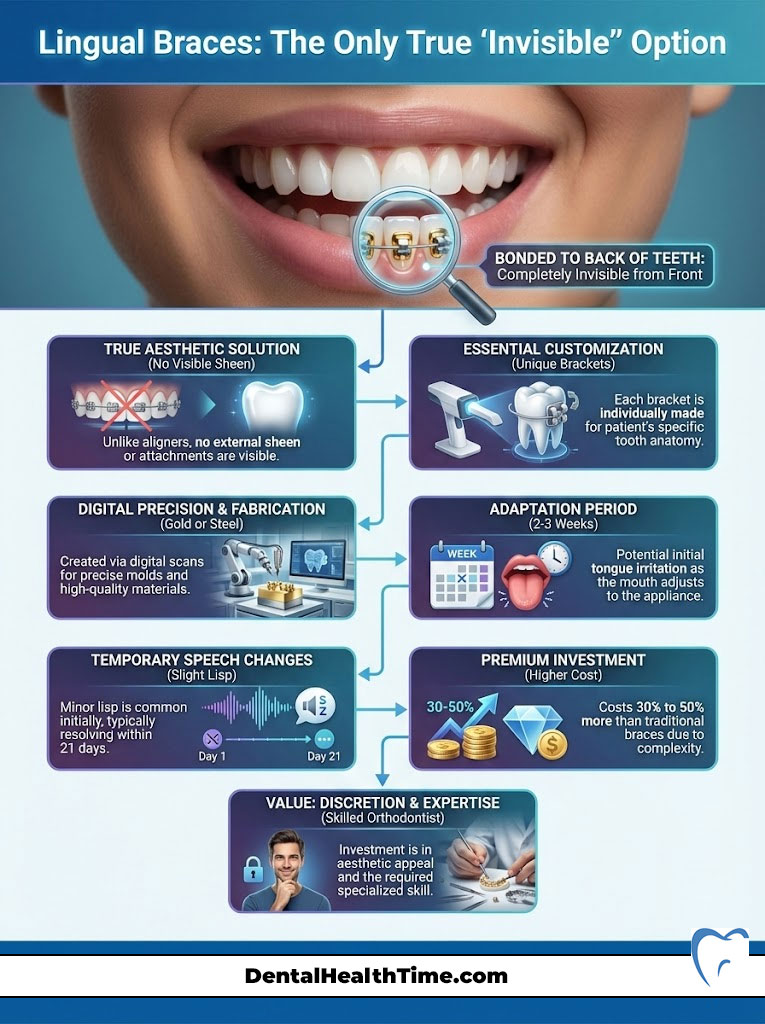
No one will know you have them. The only way to see them is if you tilt your head back and laugh. They are the ultimate aesthetic solution.
Placement Strategy and Customization
The back surface of every tooth is irregular. You cannot use generic brackets here. Lingual systems like Incognito or BRIUS are 100% customized.
We scan your teeth digitally. A laboratory then casts gold or steel alloy brackets. These are made specifically for your unique dental anatomy. The wires are also robotically bent to your prescription.
The Adaptation Period
I must be honest about the comfort level. Your tongue occupies the space where these braces sit. For the first two to three weeks, tongue irritation is significant.
Speech alterations are also common. You may have a slight lisp on “s” and “t” sounds. Most patients adapt within 21 days. But the initial phase requires resilience.
Cost Implications
When analyzing the cost, lingual is the premium tier. The lab fees alone are high due to the custom gold casting. Additionally, the chair time for the orthodontist is longer.
Working upside down behind teeth is technically demanding. Expect to pay 30% to 50% more than traditional metal braces. It is an investment in discretion.
Clear Aligner Therapy (CAT): Invisalign and Competitors
Clear aligners have revolutionized the market. They dominate the adult demographic. But are they right for everyone asking “What are the different types of braces?“? Not always.
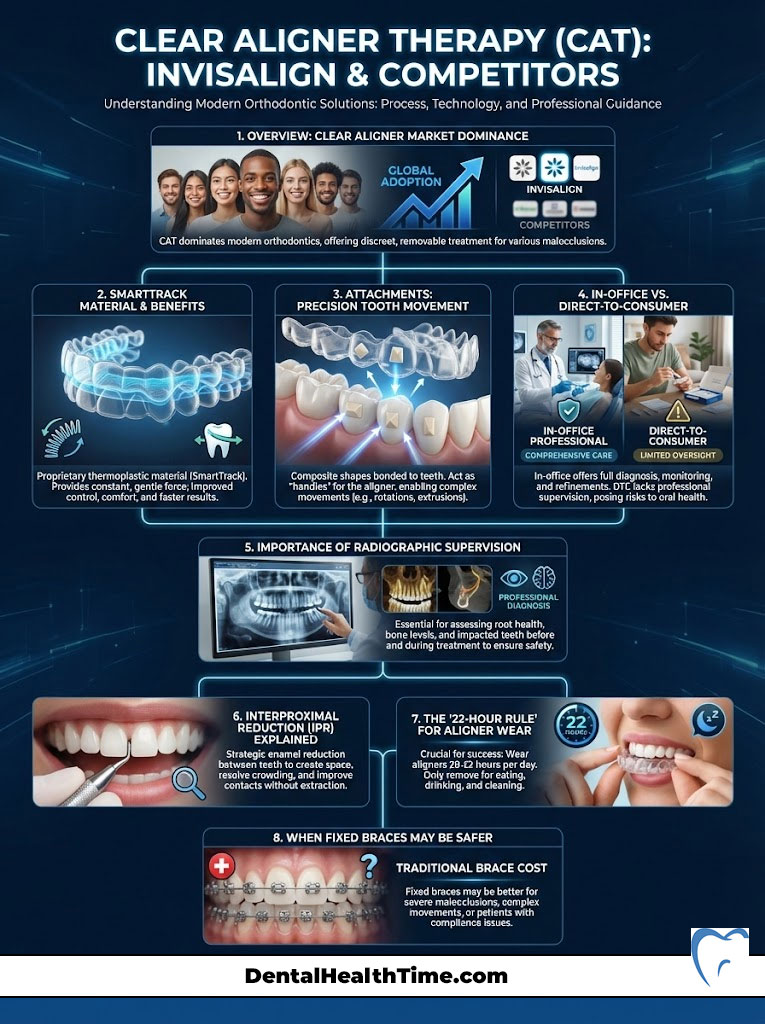
Technology: SmartTrack and Attachments
Aligners are not just smooth plastic. They are made of patented materials like SmartTrack. This material is designed to deliver constant force.
To move teeth effectively, we often bond “attachments” to your teeth. These are small bumps of composite material. They are tooth-colored. The aligner grips these bumps to rotate or extrude teeth.
In-Office vs. DTC (Direct-to-Consumer)
This is critical. Do not confuse professional aligner therapy with mail-order clubs. Direct-to-consumer aligners lack radiographic supervision.
Without X-rays, you cannot see if a tooth has short roots. You cannot see gum disease. Moving teeth in those conditions can lead to tooth loss. Always see a Board-Certified Orthodontist for aligners.
Interproximal Reduction (IPR)
With braces, we can expand the arch easily. With aligners, expansion is harder. To create space to unravel crowding, we often perform Interproximal Reduction (IPR).
This involves polishing away a fraction of a millimeter of enamel. It is done between the teeth. It is painless and safe. But it is a necessary part of the aligner process to ensure the teeth fit together.
Compliance is King
The “22-Hour Rule” is non-negotiable. You take them out to eat and brush. That’s it.
If you wear them for 18 hours, your teeth will move forward. Then they will relapse back. This “jiggling” is dangerous for the roots. If you are not disciplined, fixed braces are a safer option.
Comparison Table: Feature and Lifestyle Analysis
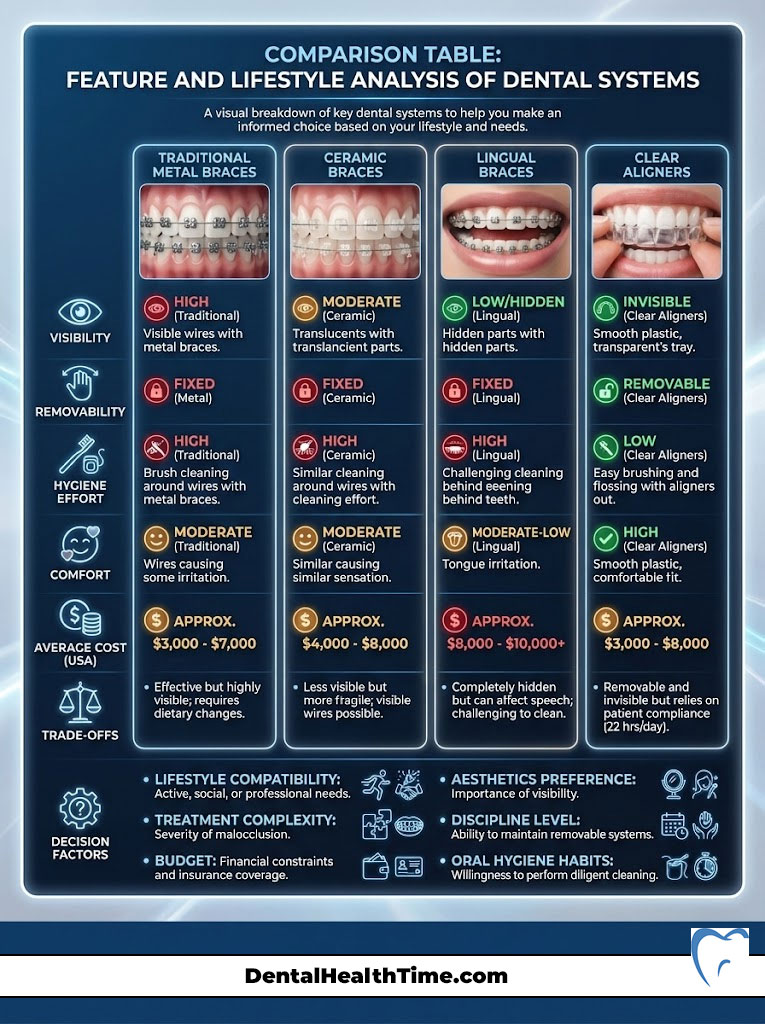
Here is a direct comparison to help you visualize the trade-offs between the systems.
| Feature | Traditional Metal | Ceramic (Clear) | Lingual (Behind Teeth) | Clear Aligners (CAT) |
|---|---|---|---|---|
| Visibility | High (Silver/Gold) | Low (Translucent) | Invisible | Very Low (Clear) |
| Removability | Fixed | Fixed | Fixed | Removable |
| Hygiene Effort | High (Threaders needed) | High (Stain management) | Very High (Hard access) | Low (Brush normally) |
| Comfort | Moderate (Cheek irritation) | Moderate (Larger bracket) | Low (Tongue irritation) | High (Smooth plastic) |
| Avg. Cost (USA) | $3,000 – $7,000 | $4,000 – $8,000 | $8,000 – $13,000 | $3,500 – $8,000 |
Beyond the Brackets: Auxiliary Appliances
Straight teeth are useless if the jaws do not fit together. This is the realm of dentofacial orthopedics. Sometimes, the brackets need help from auxiliary engines.
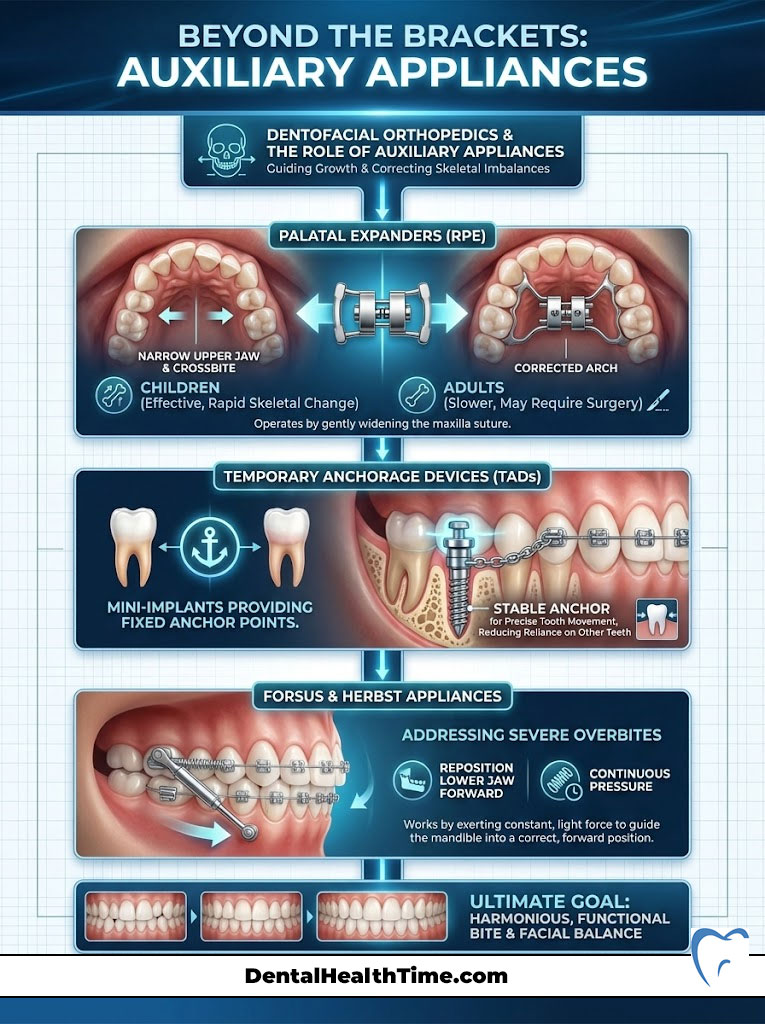
Palatal Expanders (RPE)
If the upper jaw is too narrow, we see a crossbite. We use a Rapid Palatal Expander. This device sits on the roof of the mouth.
It gently pushes the two halves of the upper jaw apart. This is most effective in children. It works best before the mid-palatal suture fuses. In adults, it often requires surgical assistance.
Temporary Anchorage Devices (TADs)
Temporary Anchorage Devices (TADs) have changed the game. These are mini-implants. They are tiny screws placed temporarily into the gum and bone.
They provide a fixed anchor point. For example, if we need to pull front teeth back, we can pull against the TAD. We do not have to pull against the back teeth. This prevents the back teeth from moving forward.
Forsus and Herbst Appliances
For severe overbites, the lower jaw is often recessed. We might install springs called Forsus or Herbst appliances. These metal rods connect the upper and lower braces.
They force the lower jaw forward into the correct position. They work 24/7. They do not rely on the patient remembering to wear rubber bands.
Clinical Efficacy by Case Type
Not all braces treat all problems equally. Here is how a Board-Certified Orthodontist matches the tool to the diagnosis.
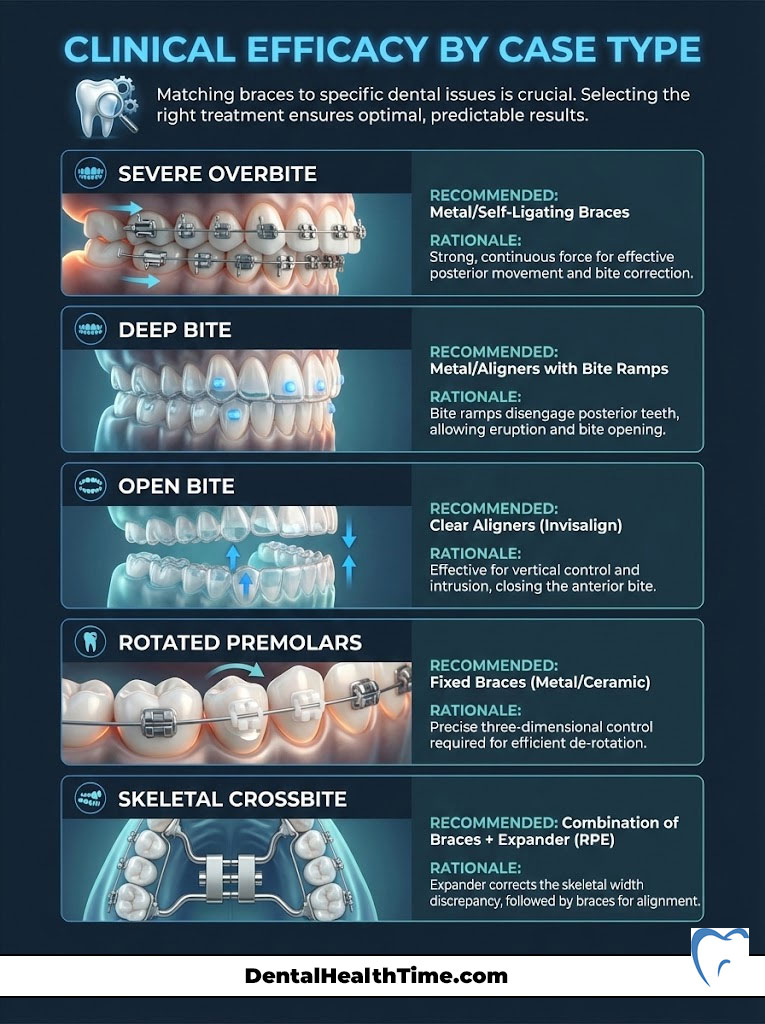
| Clinical Issue | Best Treatment Option | Why? |
|---|---|---|
| Severe Overbite | Metal / Self-Ligating | Allows use of heavy elastics and Herbst appliances. |
| Deep Bite | Metal / Aligners with Bite Ramps | Ceramic brackets may wear down opposing teeth upon contact. |
| Open Bite | Clear Aligners (Invisalign) | Plastic thickness naturally intrudes posterior teeth to close the bite. |
| Rotated Premolars | Fixed Braces (Metal/Ceramic) | Round wires rotate cylindrical teeth better than plastic. |
| Skeletal Crossbite | Braces + Expander (RPE) | Aligners alone cannot expand the skeletal suture effectively. |
Hybrid Therapy: Combining Systems
A growing trend in orthodontics is “Hybrid Therapy.” This approach acknowledges that no single system is perfect. We combine them for maximum efficiency.
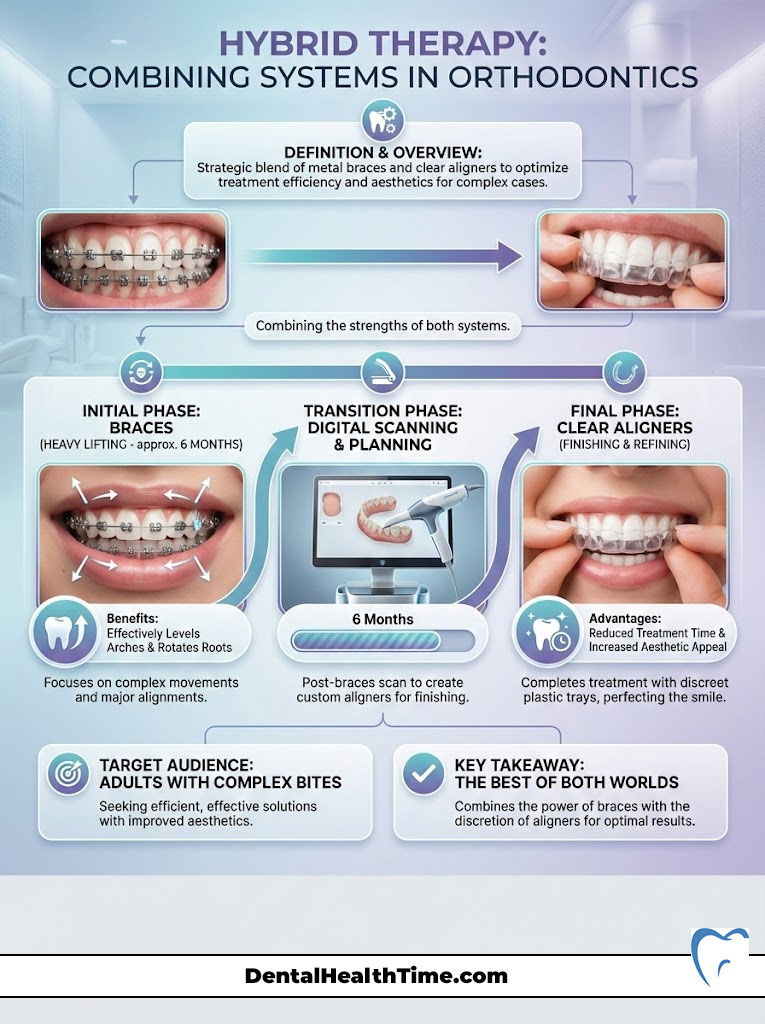
Best of Both Worlds
For example, we might start a patient with metal braces for 6 months. We use the braces to perform the heavy lifting. We level the arches and rotate the roots.
Once the difficult movements are done, we remove the braces. We then scan the patient for clear aligners. The patient finishes their treatment with plastic trays.
Cost and Time Efficiency
This method can shorten total treatment time. It utilizes the mechanical advantage of fixed brackets early on. It then offers the aesthetic advantage of aligners for the finishing phase.
It is popular with adults who have complex bites. They want the result but cannot commit to two years of metal. Ask your doctor if this is an option for you.
Treatment Phases and Lifecycle
Orthodontics isn’t always a “one-and-done” event. It often happens in phases. Understanding this timeline manages expectations.
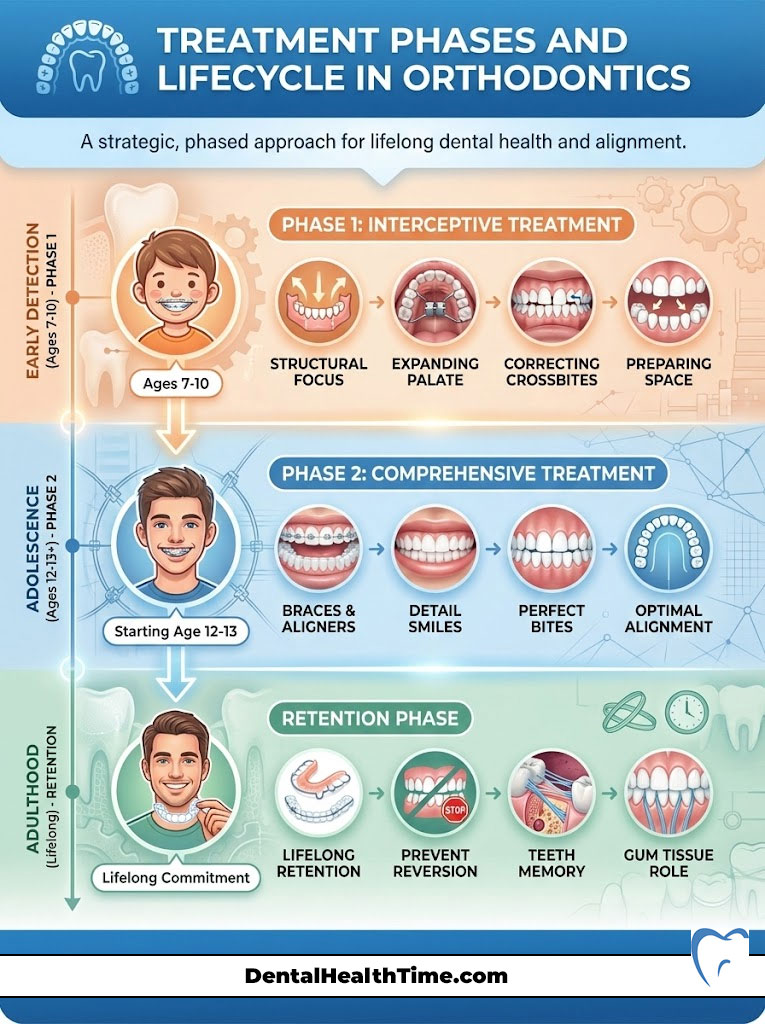
Phase 1 (Interceptive Treatment)
This occurs between ages 7 and 10. We aren’t straightening all the teeth here. We are fixing structural problems.
We might expand a narrow palate. We might fix a crossbite. We make room for adult teeth. This early intervention can prevent the need for jaw surgery later.
Phase 2 (Comprehensive Treatment)
This is the standard “braces” phase. It usually starts around age 12 or 13. This happens once all permanent teeth have erupted.
This is when we detail the smile. We perfect the bite. This is the phase most people associate with orthodontics.
Retention: The “Forever” Phase
I tell my patients: “Retention is for life.” Teeth have memory. Elastic fibers in the gums will try to pull teeth back.
They want to return to their original crooked spots. To prevent relapse, you need orthodontic retention.
- Hawley Retainers: The classic wire and acrylic plate. Durable and adjustable.
- Essix/Vivera: Clear plastic trays that look like Invisalign.
- Fixed Lingual Retainers: A permanent wire bonded behind the lower front teeth.
Cost Analysis and Insurance (USA Focus)
The cost of braces varies by geography. A case in Manhattan, NY, will cost more than in rural Ohio. This is due to overhead.

Generally, expect to invest between $3,000 and $8,000. This is a significant investment in your health.
Insurance Coverage Nuances
Dental insurance in the USA is tricky. Many plans have a “Lifetime Maximum” for orthodontics. This is usually between $1,000 and $2,000.
This is a one-time benefit. It is not annual. Crucially, many plans only cover orthodontics for dependents under age 19. This leaves adults to pay out of pocket.
Flexible Payment Structures
Most orthodontic offices function like banks. We offer interest-free monthly payment plans. These are spread over the course of treatment.
You can also use Flexible Spending Accounts (FSA). Health Savings Accounts (HSA) are also applicable. Using pre-tax dollars effectively saves you 20% to 30%.
Adult vs. Pediatric Orthodontics
Is treating a 40-year-old different from treating a 14-year-old? Absolutely. The biology changes as we age.
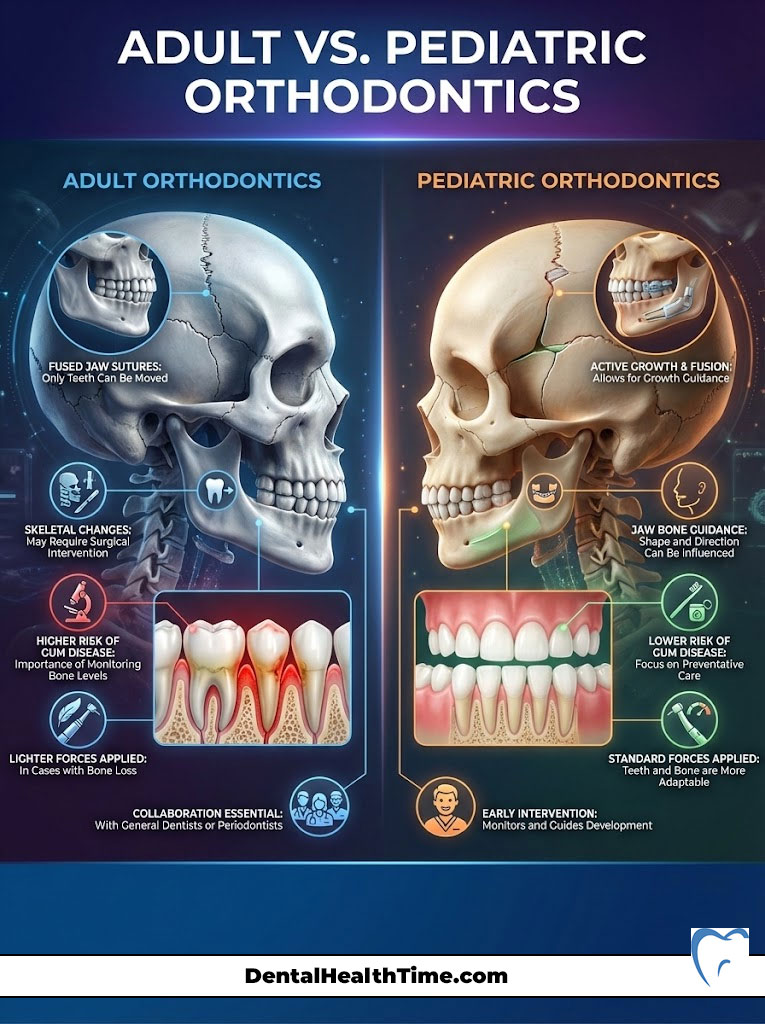
The Fusion of Sutures
In children, the jaw bones are not fully fused. We can guide growth. We can expand the palate easily.
In adults, the sutures are fused. We cannot grow bone. We can only move teeth within the existing bone. Skeletal changes in adults often require surgery.
Periodontal Health
Adults are more prone to gum disease. We must monitor bone levels closely. If an adult has bone loss, we must apply lighter forces.
We move teeth slower to protect the periodontium. Collaboration with a general dentist or periodontist is often required.
Summary & Key Takeaways
We have covered a lot of ground. When you revisit the question, “What are the different types of braces?” remember that there is no single “best” brace.
There is only the best brace for you. Traditional metal braces offer unmatched control for complex cases. Ceramic braces provide a blend of strength and aesthetics.
Lingual braces offer total invisibility for those willing to endure the adaptation period. Clear aligners offer flexibility and hygiene benefits for disciplined patients.
My final advice? Do not shop for a commodity. Shop for a doctor. The skill of the Board-Certified Orthodontist designing your smile matters far more than the brand of bracket.
They glue the bracket to your teeth, but they design the outcome. Schedule a consultation. Get a CBCT scan. Choose the path that ensures your smile is not just beautiful, but healthy and stable for a lifetime.
Frequently Asked Questions
What are the main clinical categories of orthodontic braces?
Orthodontics typically utilizes four primary categories: traditional metal, translucent ceramic, lingual (behind the teeth), and clear aligner therapy. Each system serves a specific clinical purpose based on the patient\’s malocclusion, biological needs, and lifestyle requirements as determined by a Board-Certified Orthodontist.
How do metal braces differ from ceramic braces in terms of durability?
While ceramic braces offer superior aesthetics using tooth-colored polycrystalline alumina, they are more brittle than stainless steel and prone to fracturing under high masticatory pressure. Metal braces remain the gold standard for durability and are often required for heavy-force movements like correcting deep bites or severe skeletal discrepancies.
Are clear aligners like Invisalign as effective as traditional metal braces for complex cases?
Clear aligners are excellent for mild to moderate crowding, but fixed appliances provide more precise control over root torque and complex rotations of cylindrical teeth. For surgical cases or severe malocclusions, an orthodontist may recommend metal braces or a hybrid therapy approach to ensure stable, long-term functional results.
What are lingual braces and why are they considered the only truly invisible option?
Lingual braces are custom-fabricated brackets bonded to the posterior (tongue-side) surface of the teeth, making them completely hidden from view even during close conversation. Because they require specialized technical expertise and custom gold or steel alloy casting, they represent the premium tier of aesthetic orthodontic solutions.
How does the biological process of bone remodeling allow teeth to move?
Teeth move through a physiological process where pressure triggers osteoclasts to break down bone in the path of movement, while tension stimulates osteoblasts to build new bone behind the tooth. This inflammatory response must be carefully managed with light, constant forces to avoid root resorption, which is the permanent shortening of the tooth roots.
What is the typical cost range for orthodontic treatment in the United States?
In the US, orthodontic treatment generally ranges from $3,000 to $8,000 depending on the complexity of the case, geographic location, and the type of appliance used. Many dental insurance plans offer a one-time lifetime maximum benefit, and most clinics provide interest-free monthly payment plans to help manage the investment.
Why do orthodontists use CBCT 3D imaging instead of traditional impressions?
Modern practices utilize Cone Beam Computed Tomography (CBCT) to provide 3D visualizations of tooth roots, bone density, and the airway, which traditional 2D X-rays cannot offer. This technology, often paired with iTero digital scanners, eliminates the need for uncomfortable putty impressions while significantly increasing diagnostic precision and treatment safety.
Can ceramic braces stain your teeth during treatment?
High-quality ceramic brackets themselves are impervious to staining from coffee or food; however, the clear elastic ligatures used to secure the archwire can discolor over time. These bands are replaced at every adjustment appointment, and patients can opt for self-ligating ceramic systems to eliminate the use of stain-prone elastics entirely.
What are self-ligating braces and how do they reduce friction during tooth movement?
Self-ligating systems, such as Damon braces, use a specialized built-in “sliding door” mechanism instead of rubber bands to secure the archwire. This creates a low-friction environment (passive ligation) that allows teeth to move more freely, which can lead to faster initial leveling and a more comfortable experience for the patient.
At what age should a child have their first orthodontic screening according to the AAO?
The American Association of Orthodontists (AAO) recommends a child’s first orthodontic screening by age seven. This allows for “interceptive treatment” to guide jaw growth and manage space for erupting permanent teeth, which can prevent the need for more invasive procedures like extractions or jaw surgery later in life.
What are Temporary Anchorage Devices (TADs) and when are they necessary?
Temporary Anchorage Devices (TADs) are mini-implants temporarily placed into the bone to act as a fixed anchor point for specific tooth movements. They allow orthodontists to perform complex biomechanical tasks, such as closing large gaps or correcting severe intrusions, without causing unwanted “reactive” movement in the surrounding teeth.
Why is wearing a retainer essential after completing orthodontic treatment?
Retention is a lifelong phase because teeth have a natural tendency to relapse toward their original positions due to the memory of elastic gum fibers. Whether using a Hawley, Essix, or a fixed lingual wire, consistent retainer wear is the only way to protect your investment and maintain a stable, healthy smile permanently.
Disclaimer
This article is for informational purposes only and does not constitute medical advice. Orthodontic treatment is highly individualized and involves biological risks such as root resorption. Always consult a Board-Certified Orthodontist for a comprehensive diagnosis and a treatment plan tailored to your specific bone structure and dental health.
References
- American Association of Orthodontists (AAO) – aaoinfo.org – Official guidelines on orthodontic treatment timing and appliance types.
- American Board of Orthodontics (ABO) – americanboardortho.com – Standards for board certification and clinical excellence in orthodontics.
- Journal of Clinical Orthodontics (JCO) – jco-online.com – Peer-reviewed studies on the efficacy of self-ligating vs. traditional brackets.
- National Center for Biotechnology Information (NCBI) – pubmed.ncbi.nlm.nih.gov – Research on the biological mechanisms of bone remodeling and root resorption.
- Journal of Evidence-Based Dental Practice – Clinical comparison of clear aligner therapy versus fixed orthodontic appliances.
11 thoughts on “What Are the Different Types of Braces? A Complete Guide”